Idea in Brief
As we move through 2024, 16 years since the WHO Health System framework was introduced, it is time to put its impact on the Sustainable Development Goals (SDG) 2030 agenda front and center in national, regional and global health conversations. This dialogue should spark a reimagining of our health systems for the future.
Here’s why this discussion is both urgent and crucial. Consider the Service Coverage Index, which tracks SDG indicator 3.8.1. Africa’s average score of 48 starkly reveals enormous gaps in healthcare access. While there’s been commendable progress in areas like child health and the fight against infectious diseases – thanks largely to investments from development agencies – other areas, such as maternal health, still fall far short of SDG targets. Moreover, the rise of non-communicable diseases threatens to undo these hard-won gains. In the face of ongoing global challenges like pandemics, climate change, and resource constraints, there is an urgent need to evolve toward a new health system framework – Health Systems 2.0 – designed to create resilient, impactful health systems.
This article proposes a blueprint for Health Systems 2.0, built on three foundational theories: systems thinking, human-centered design, and adaptive leadership. Systems thinking emphasizes the interdependence of health sub-systems and calls for a holistic approach that considers local socio-political contexts. Health Systems 2.0 conceptualizes health systems as a combination of inputs, processes – including the WHO’s six building blocks – population health outputs, informational feedback loops, and governance or control mechanisms, all operating within a complex environment. Adaptive leadership is key to strengthening health systems by distinguishing between technical problems and adaptive challenges and guiding change through an empathetic, inclusive approach. Human-centered design ensures that solutions are tailored to the specific needs and contexts of the communities they serve.
Health systems often stagnate in inefficient equilibrium, delivering sub-optimal outcomes. However, by integrating systems theory, adaptive leadership, and human-centered design, we can optimize system resilience and health outcomes, even in resource-constrained settings facing threats like climate change and pandemics. Transforming health systems is a collective effort, requiring the collaboration of the World Health Organization, governments, development agencies, global health organizations, civil society, local communities, academics, and health workers.
Why Re-imagine Health Systems?
As we approach 2024, it is crucial to reflect on the WHO Health System framework and its influence on health system resilience and population health outcomes. With just six years left until the 2030 SDG deadline, the effectiveness of this framework warrants open discussion.
Upcoming global gatherings like the Summit of the Future in September 2024, the Global Symposium on Health Systems Research, the World Health Assembly, the United Nations General Assembly, the World Health Summit, the Africa Health Agenda International Conference, and the Conference on Public Health in Africa can provide vital platforms for health leaders and stakeholders to review and advance the framework, accelerating progress towards SDG 3. It would be highly beneficial if the organizers of these events enhanced the depth of upcoming discussions by incorporating sessions that re-examine health systems from a framework perspective – rather than focusing solely on individual building blocks – to advance health systems theory and practice.
Health systems are the means to a crucial end: achieving universal health coverage and improving population health. The Service Coverage Index tracked as SDG indicator 3.8.1, measures the effectiveness of health systems strengthening initiatives in any country or region. However, the index reveals a troubling disparity in healthcare access across different regions. For instance, in Africa, the average score of 48 on a scale of 1 to 100 highlights significant gaps in healthcare access that affect hundreds of millions of people.
Despite commendable progress, such as halving child mortality in Africa between 2000 and 2019, serious challenges remain. Maternal health outcomes are particularly alarming, with maternal mortality rates far off track from SDG targets. Additionally, the rising burden of non-communicable diseases threatens to reverse many of the gains made on the continent.
This mixed reality signals the pressing need for a paradigm shift. We need to evolve towards a health system designed for people, one that is capable of delivering meaningful impact amidst contemporary global challenges like climate change and pandemics. It is time to redefine the current health system framework, moving towards its next iteration – Health Systems 2.0 – focusing on resilience and impact.
Theoretical Foundations for Health Systems 2.0
In building Health Systems 2.0, I propose a design methodology that seamlessly integrates three key theories: systems thinking, human-centered design, and adaptive leadership.
(a) Systems Thinking
Originating from Ludwig von Bertalanffy [6], Systems Theory highlights the interdependence of system components, including challenges, and underscores the need for holistic solutions that address stakeholder needs. Researchers such as Paina and Peters [7], along with Braithwaite J. et al. [8], argue that adopting a complex adaptive systems framework is essential for successfully scaling health system interventions. This approach emphasizes the importance of understanding local nuances, social practices, and the interconnected nature of healthcare while promoting transparent, adaptive problem-solving. When people are part of a system, complexity increases due to the unpredictability of human emotions and needs. This often leads to unexpected events that can disrupt the system’s functioning.
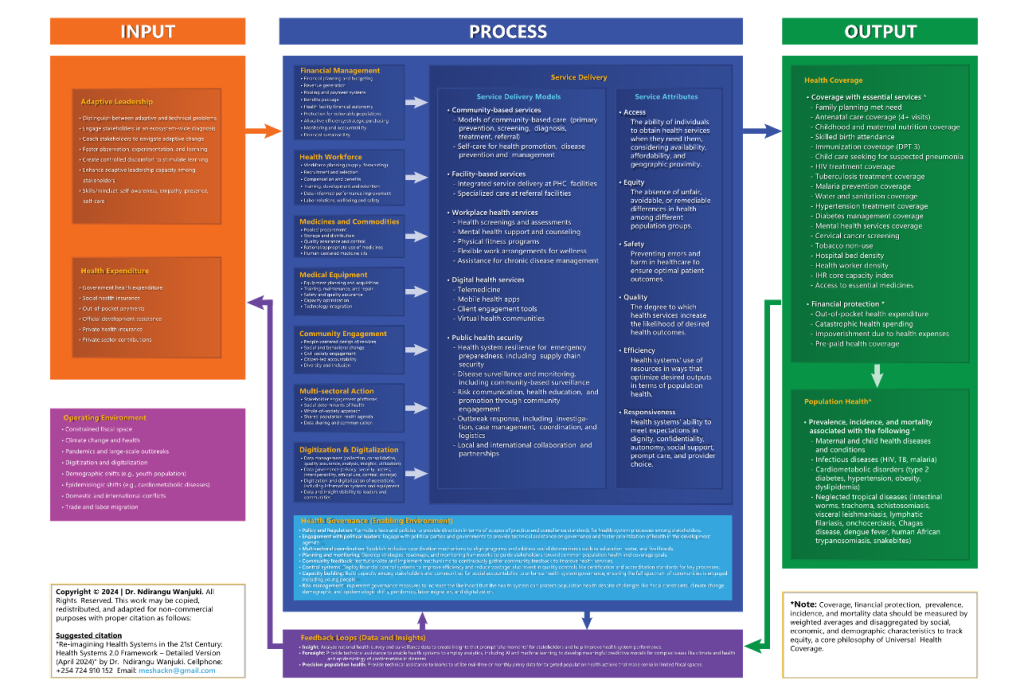
Figure 1: Health Systems 2.0 Framework Founded on System Design, Human-Centered Design, and Adaptive Leadership (Simplified Version)
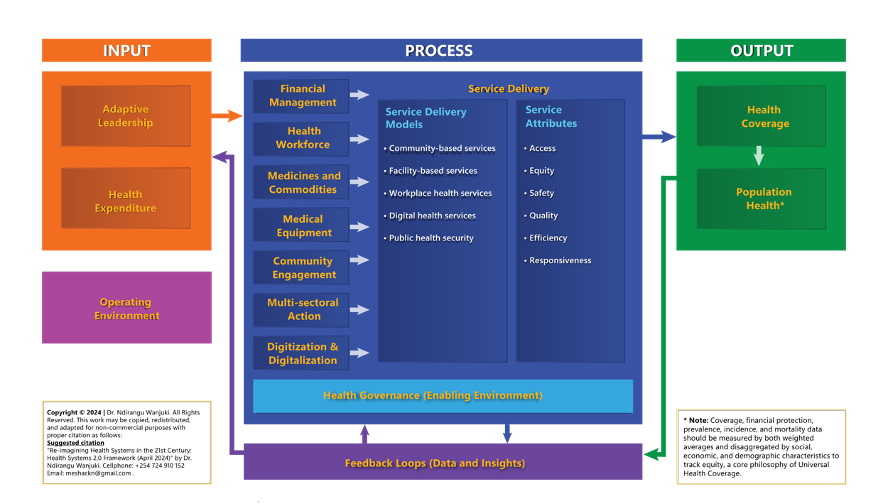
In this paper, Health Systems 2.0 is defined by a framework that includes inputs, processes, outputs, feedback loops, governance as controls, and an increasingly complex operating environment (see Figure 1 for a simplified version of HS 2.0 and Annex 1 for the detailed version). This framework develops on the six building blocks of the 2007 WHO health systems framework, integrating them within the context of systems thinking.
Input
In Health Systems 2.0, inputs revolve around adaptive leadership and funding. Adaptive leadership provides vision, direction, and order while navigating the myriad challenges and opportunities within the health ecosystem. Funding, viewed through the lens of total health expenditure from a blended financing perspective, is equally crucial. When health systems fail to deliver the expected population health benefits despite significant efforts to improve processes, it is often due to flaws in these inputs – either a lack of adaptive leadership or grossly inadequate funding allocation.
Process
The processes in Health Systems 2.0 operate across eight domains, each functioning as a sub-system that interacts towards the common goal of producing health. These domains include financial management, the health workforce, medicines and commodities, medical equipment, community engagement and multi-sectoral action to address social determinants of health (involving sectors like education, gender, environment, agriculture, water and sanitation), digitization and digitalization, and the delivery of promotive, preventive and curative services. To achieve the desired population health outcomes, services must be delivered in a way that is convenient and contextually appropriate for communities. This involves deploying fit-for-purpose delivery models, including community-based services, facility-based services, workplace health services, digital health services, and public health security. A useful way to assess services in the short term is through six key lenses that matter to communities: access, equity, safety, quality, efficiency, and responsiveness.
Outputs
Outputs in Health Systems 2.0 focus on health system performance, measured by coverage of essential services, financial protection and, ultimately, population health. Managers at sub-national levels, such as districts and counties, should concentrate their efforts on organizing the eight sub-systems to optimize performance concerning these three outputs within their specific settings and contexts.
Feedback Loops
Feedback loops in Health Systems 2.0 involve leveraging insights and foresight derived from digitized data to guide health systems toward precision population health. In this context, precision population health enables practitioners to discover and implement minimalistic system improvement pathways that are both efficient and data-driven, focusing on addressing prioritized health needs. This approach could allow health systems, particularly in fiscally constrained regions like much of Africa, to achieve meaningful results despite limited resources.
Governance
Governance in Health Systems 2.0 provides enabling environments for effective health systems to develop, thrive, and prosper. This requires thoughtful investment in several key areas: policies and regulations, engagement with the political class, mechanisms for multi-sectoral coordination, planning and monitoring (including timely community feedback), financial and quality control systems, building governance capacity among stakeholders, and implementing risk mitigation measures, particularly in response to trends or factors in the operating environment described in the next paragraph.
Health Systems 2.0 must remain open and adaptive to prevailing environmental factors and trends. This paper identifies eight such forces that influence health systems: constrained fiscal space, climate change and its impact on health, pandemics and large-scale outbreaks, digitization and digitalization, demographic shifts (such as youth population growth), epidemiologic shifts (such as the rise in cardiometabolic diseases), domestic and international conflicts, and trade and labor migration.
As Straub [9] argues, managers often underestimate the complexity of systems in their efforts to simplify work, which can limit their ability to maintain control. By applying the principles of Health Systems 2.0 – combining systems theory with human-centered design and adaptive leadership – health sector managers can strategically focus their efforts on the most effective leverage points within one or more of the eight key processes. This approach can lead to affordable improvements in health outcomes, even in resource-limited settings like Africa and other developing regions. For instance, Rwanda [10] and Ethiopia [11] have successfully improved health outcomes by strengthening community health worker programs, while Malawi achieved better surgical outcomes through task-shifting to clinical officers [12].
Systems Theory
While Systems Theory has proven successful in many cases, it is not a panacea. Health systems can sometimes find themselves in an “inefficient equilibrium”, where processes across one or more of the eight domains or sub-systems appear stable but ultimately fail to deliver the expected improvements in population health outcomes, despite significant effort.
By integrating Systems Theory with adaptive leadership – essential for recognizing inefficiencies and driving change – and human-centered design, which prioritizes the needs of people across all eight process domains, it is possible to create more efficient systems that are optimized to deliver better population health outcomes.
(b) Adaptive Leadership
Adaptive leadership is a crucial component of Health Systems 2.0. Presidents, prime ministers, and other national leaders must prioritize appointing individuals who practice adaptive leadership to key roles, such as the Minister for Health or Director of Medical Services. This approach should also extend to subnational leaders, including ministers or directors in charge of health at the state, county, district, or provincial level.
Health Systems 2.0 underscores the importance of recognizing adaptive challenges distinct from technical problems, as confusing the two often leads to leadership failures. Adaptive leadership involves distinguishing between adaptive challenges, which require leadership, and technical problems, which do not [13]. Heifetz et al. emphasize that technical problems, such as a surgeon performing an operation, can be resolved with existing knowledge and procedures. In contrast, adaptive challenges – such as persistently high maternal mortality rates, rising teenage pregnancy rates, or the unrecognized pandemic of cardiometabolic diseases – exist within a complex ecosystem of individuals and organizations with diverse interests, values, and motivations.
Leading through adaptive challenges involves empathetically helping people learn and adjust to change. This involves managing loss, fostering a culture of observation, experimentation, and learning, and creating just enough discomfort to stimulate growth while maintaining a supportive environment. In addition, adaptive leadership entails developing adaptive solutions within a diverse ecosystem of stakeholders.
To address adaptive challenges, practitioners of adaptive leadership engage in a diagnostic process to understand the problem’s ecosystem. This process includes identifying stakeholders, appreciating their perspectives, clarifying their desired outcomes, recognizing positive deviance where parts of the system function well [14], and coaching stakeholders to enhance their adaptive leadership capacities. This approach helps drive change while preserving what is already working as a foundation.
The practice of adaptive leadership demands self-awareness, presence, deep listening, genuine engagement with others, and self-care to prevent exhaustion and burnout.
(c) Human-Centered Design
Human-centered design, also known as people-centered design, prioritizes creating solutions that address the specific needs and contexts of communities rather than catering to the preferences of the designer [15, 16]. This approach involves deeply empathizing with communities to understand their unique challenges, clearly defining the problems, ideating and prototyping potential solutions, testing these solutions with the communities, and iterating based on the feedback received. By following this process, health solutions are tailored to genuinely meet community needs in aspects such as access, quality, affordability, and responsiveness.
Successful examples of human-centered design within health systems include the Aravind Eye Care System in India [17, 18], the Kimormor One-Stop-Shop Outreach Model in Kenya, which integrates animal and human health services [19, 20], and low-cost, solar-enabled mobile clinics that deliver COVID-19 vaccines and other essential services to remote or hard-to-reach areas of Kenya [21]. Other examples include the surgical training program for clinical officers in Malawi [22], the Better Immunization Data initiative in Tanzania and Zambia [23], and Rwanda’s success in maternal health, partly attributable to community-based interventions [24].
Reimagining Health Systems: A Game of Stakeholders
Shaping the future of health systems is a collective responsibility, and everyone has a role to play. UN bodies like the WHO and regional entities must continue their roles in facilitating, mediating and providing technically sound guidance to help countries customize their health systems. Platforms like the World Health Assembly, the UN General Assembly and the Summit of the Future offer prime opportunities to discuss the evolution from the WHO Health Systems Framework of 2017 to more contemporary models. Health Systems 2.0 is a prime example of such an evolution. The WHO should consider convening a high-level dialogue on “The Health System of the Future” to propel this conversation forward.
Governments are in a strong position to embrace adaptive leadership and allocate reasonable amounts of funds, which are foundational inputs for building robust health systems. Bilateral and non-UN multilateral development organizations, global health partnerships and philanthropic foundations would benefit from reimagining their support to strengthen adaptive leadership and data-driven performance improvements within health systems. Performance improvement should focus on health system outputs, namely service coverage, financial protection and population health. Civil society, representing diverse communities, needs to better organize to advocate for the early implementation of evidence-based and effective health system models, including iterations like Health Systems 2.0. Facilitating strategic discussions with government ministers, WHO and philanthropic foundations during key global health events is crucial. Academics specializing in health should contribute to these discussions by presenting evidence on the effectiveness of the current health systems framework and potential Health Systems 2.0 adaptations, particularly in lower-income countries.
Health workers must continue to demonstrate excellence at the frontline, using adaptive leadership to address persistent health challenges. The persistence of a health challenge at the population level is perhaps the clearest indicator of an adaptive challenge, as opposed to a technical one.
By re-envisioning health systems through the lenses of Systems Theory, human-centered design and adaptive leadership, we can enhance system resilience and sustainably improve health outcomes, even in the face of economic constraints and global threats like climate change and pandemics.
In closing, I thank you for reading this opinion piece and encourage you to identify adaptive challenges in your work and practice proactive leadership to address them, regardless of your position of authority.
References
- World Health Organization. Everybody’s Business: Strengthening health systems to improve health outcomes – WHO’s framework for action. 2007; 44.
- https://data.unicef.org/resources/levels-and-trends-in-child-mortality-2021/Levels & Trends in Child Mortality. Report 2021. New York: United Nations Children’s Fund (UNICEF). 2021.
- Sharrow D, Hug L, You D, Alkema L, Black R, Cousens S, et al. Global, regional, and national trends in under-5 mortality between 1990 and 2019 with scenario-based projections until 2030: a systematic analysis by the UN Inter-agency Group for Child Mortality Estimation. Lancet Glob Health. 2022 Feb;10 (2):e195–206.
- Trends in maternal mortality 2000 to 2020. Geneva: World Health Organization; 2023.
- Gitahi G, Wanjuki N. Placing people at the heart of African health systems. BMJ. 2023 Apr 13; p734.
- Bertalanffy LV. General System Theory; Foundations, Development, Applications. New York: G. Braziller; 1969.
- Paina L, Peters DH. Understanding Pathways for Scaling up Health Services Through the Lens of Complex Adaptive Systems. Health Policy Plan. 2012 Aug 1; 27(5):365–73.
- Braithwaite J, Churruca K, Long JC, Ellis LA, Herkes J. When complexity science meets implementation science: A theoretical and empirical analysis of systems change. BMC Med. 2018 Dec;16(1):63.
- Straub R. Why Managers Haven’t Embraced Complexity. Harvard Business Review. 2013. https://hbr.org/2013/05/why-managers-havent-embraced-c. Accessed 15/3/2024
- Binagwaho A, Farmer PE, Nsanzimana S, Karema C, Gasana M, De Dieu Ngirabega J, et al. Rwanda 20 years on: Investing in life. The Lancet. 2014 Jul; 384 (9940):371–5.
- Medhanyie A, Spigt M, Kifle Y, Schaay N, Sanders D, Blanco R, et al. The role of health extension workers in improving utilization of maternal health services in rural areas in Ethiopia: A cross sectional study. BMC Health Services Research. 2012 Dec;12(1):352.
- Gajewski J, Borgstein E, Bijlmakers L, Mwapasa G, Aljohani Z, Pittalis C, et al. Evaluation of a surgical training programme for clinical officers in Malawi. Br J Surg. 2019 Jan 8;106(2):e156–65.
- The Practice of Adaptive Leadership: Tools and Tactics for Changing Your Organization and the World by Ronald Heifetz, Alexander Grashow and Marty Linsky. Pers Psychol. 2010 Mar;63(1):255–8.
- Pascale R, Sternin J, Sternin M. The Power of Positive Deviance: How Unlikely Innovators Solve the World’s Toughest Problems. Harvard Business Press. 2010.
- IDEO.org. The Field Guide to Human-Centered Design. 2015. Canada. IDEO.
- Huffman K. The key to better primary health care? Human-centered design. 2019. https://www.path.org/our-impact/articles/key-better-primary-health-care-human-centered-design/. Accessed 12/03/2024
- Lewallen S, Thulasiraj RD. Eliminating cataract blindness – how do we apply lessons from Asia to sub-Saharan Africa? Glob Public Health. 2010 Nov;5 (6):639–48.
- Saqib, N. & Mathu, A. A. (2024). Frugal Business Model Innovation in an Indian Emerging Market: A Case Study of Aravind Eye Care System. In V. Gupta (Ed.), Fostering Global Entrepreneurship Through Business Model Innovation (pp. 184-205). IGI Global. https://doi.org/10.4018/978-1-6684-6975-0.ch007
- Amref. Where families and their animals are treated in one clinic (Reported by Angela Oketch, Nation Media Group). 2021. https://newsroom.amref.org/news/2021/01/where-families-and-their-animals-are-treated-in-one-clinic/. Accessed 12/03/2024
- Amref. One Health Approach Strengthens Human and Animal Health in Turkana, Kenya (Reported by Kevin Majoni, Communications Lead, USAID Imarisha Jamii). 2024. https://newsroom.amref.org/blog/2024/03/one-health-approach-strengthens-human-and-animal-health-in-turkana-kenya/. Accessed 17/08/2024
- Amref. Ministry of Health, Kenya, in Partnership with Amref Health Africa and AstraZeneca, Rolls out Mobile Clinics to Boost Covid Vaccines Uptake. 2022. https://newsroom.amref.org/news/2022/07/moh-rolls-out-mobile-clinics-to-boost-covid-vaccines-uptake/. Accessed 12/03/2024
- Gajewski J, Borgstein E, Bijlmakers L, Mwapasa G, Aljohani Z, Pittalis C, et al. Evaluation of a surgical training programme for clinical officers in Malawi. Br J Surg. 2019 Jan 8;106(2):e156–65.
- Mvundura M, Di Giorgio L, Vodicka E, Kindoli R, Zulu C. Assessing the incremental costs and savings of introducing electronic immunization registries and stock management systems: evidence from the better immunization data initiative in Tanzania and Zambia. Pan Afr Med J. 2020 Feb 12;35(Suppl 1):11. doi: 10.11604 pamj.supp.2020.35.1.17804. PMID: 32373262; PMCID: PMC7195915.
- Bucagu M. Improving maternal health in Rwanda: The role of community-based interventions: a systematic review (2005-2015). J Community Med Health Educ. 2016;6:434. doi:10.4172/2161-0711.1000434.
Annex 1: Health Systems 2.0 Framework Founded on System Design, Human-Centered Design, and Adaptive Leadership (Detailed Version)