Idea in Brief
The 2023 Universal Health Coverage (UHC) global monitoring report underscores an urgent need for health systems reform worldwide, particularly in the pursuit of achieving UHC by 2030. Despite some progress, recent post-MDG (Millennium Development Goals) era stagnation in the UHC trajectory has exposed significant challenges in implementing Primary Health Care (PHC), calling for leadership and health system innovation. With approximately 4.5 billion people lacking full access to essential health services and one billion individuals facing crippling out-of-pocket expenses, the need for a new health system-strengthening approach is both pressing and undeniable.
In response, the author proposes a Health Systems 2.0 framework and advocates for stakeholders to embrace eight critical practices to disrupt the current stagnation and drive meaningful improvements in population health. Central to this framework is the prioritization of PHC, which could potentially deliver 90% of UHC interventions and save 60 million lives. Health Systems 2.0 practices include establishing a clear and shared mission focused on improving population health, supported by the application of leadership and funding as core and essential system inputs. Further, it emphasizes the importance of investing in eight interdependent, people-centered processes: finance management, human resources, medicines and commodities, medical equipment, community engagement, multi-sectoral collaboration, digitization and digitalization, and integrated health services through models of delivery that are convenient for communities.
To foster efficient stability or equilibrium in the context of health systems, Health Systems 2.0 practice prioritizes the strengthening of health governance as a foundation for system control, coupled with leveraging real-time data through precision population health strategies to make cost-effective improvements while adapting to environmental factors like climate change, pandemics, and digitalization. For all this to hold, stakeholders are urged to embrace the practice of adaptive leadership irrespective of their titles or positions and adopt a reformist mindset committed to continuous system improvement and innovation, crucial for overcoming existing challenges and pushing the boundaries of what is possible in global health.
The adoption of these eight Health Systems 2.0 practices offers hope for finding pathways to reorient health systems using the PHC approach and making faster progress towards the 2030 UHC goal. Embracing the practices could bring more meaning to our work while resonating with and fostering the trust of communities, who are the reason health systems exist.
Urgent Call for Health Systems Reform
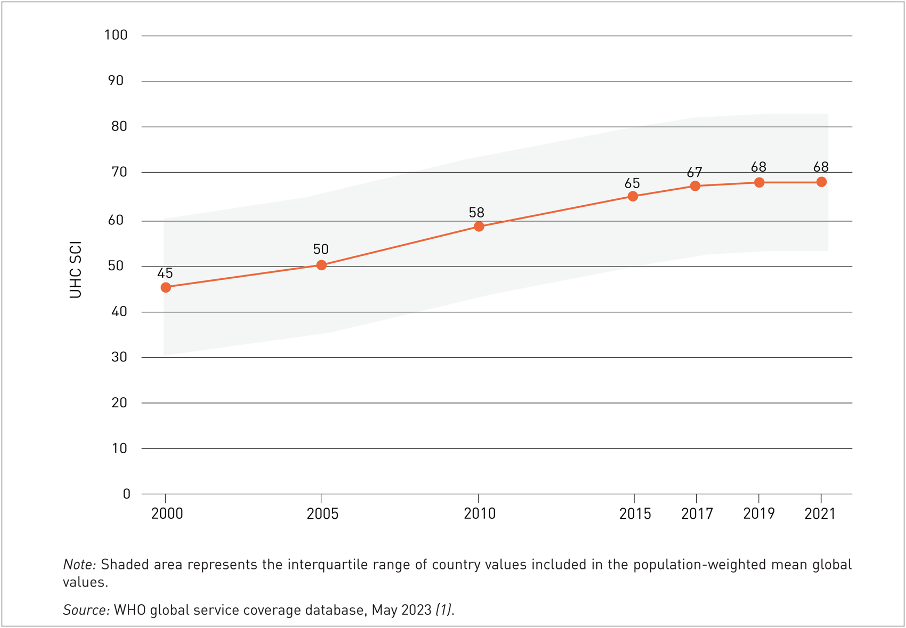
UHC means that all people have access to the full range of quality health services they need, when and where they need them, without financial hardship. The 2023 UHC global monitoring report shows that the world is off track to achieve the Universal Health Coverage SDG target 3.8 by 2030. Although the UHC index improved from 45 to 68 out of 100 between 2000 and 2021, progress slackened from 2015 and has stagnated since 2019 (Figure 1). Around 4.5 billion people lack full access to essential health services, and one billion face severe out-of-pocket health expenses. The stagnation is due to gaps in Primary Health Care (PHC) implementation, insufficient funding and the impact of COVID-19. Consequently, WHO recommends reorienting health systems using a PHC approach.
In Africa, where health spending averages US$54 per capita, leadership and health system innovation are needed to drive this reorientation. This calls for a new health systems framework, and the author proposes such a framework to stimulate discussion (see Annex 1 for a simplified Health Systems 2.0 framework and Annex 2 for a detailed version). He suggests that those wishing to contribute to PHC-focused health systems reform, whom he calls Health Systems 2.0 practitioners, can reimagine their mental models about health systems and consciously implement eight synergistic HS 2.0 practices to increase the likelihood of positively disrupting the stagnated UHC trajectory and achieving a durable population-level impact.
Practice #1 – Begin With a Shared Mission of Improving Population Health
Health Systems 2.0 (HS 2.0) practitioners, driven by a sense of purpose, begin by defining the desired impact, such as improving the UHC index from X to Y or reducing maternal mortality from A to B within five to ten years, as often outlined in government strategies. They assist governments in convening stakeholders to support a shared, people-centered agenda built on affordable pathways that can advance progress toward population health goals. These impact-level goals serve as the outputs of a working health system.
By setting and pursuing coverage or population health goals as the ultimate output of health systems, they help health systems avoid the ‘inefficient equilibrium’ trap affecting many nations, currently evidenced by the stagnated trajectory of the UHC index. One hallmark of HS 2.0 practitioners is their effort to assist governments in convening and rallying stakeholders toward a shared coverage and population health improvement agenda. During election cycles, you’ll find HS 2.0 practitioners engaging various political parties to include financing, governance, coverage and population health commitments in their manifestos. They guide or coach others to recognize that health systems serve the purpose of improving population health. This improvement is assessed through scheduled national surveys or real-time proximate estimates from routine health information and surveillance systems. By fostering this understanding, HS 2.0 practitioners inspire their peers to leverage available resources and direct their efforts through minimalist pathways that can advance population health. As you will notice in Practice #4, finding such lean pathways is a lifeline for countries with markedly constrained fiscal spaces.
Practice #2 – Prioritize Leadership and Funding as Core Inputs
Health Systems 2.0 has two pivotal inputs – money and leadership – which, if applied effectively, are sufficient to achieve the desired population health impact. Effective leadership enables the management of available financial resources in ways that optimize sub-systems such as human resources, medical commodities, equipment, community engagement and multi-sectoral action as described in Practice #3, to synergistically operate in ways that deliver coverage and population health results. When health systems fail to deliver population health despite significant, well-intentioned efforts, the root cause and lesson often lie in the inputs, specificallya lack of adaptive leadership and/or grossly inadequate funding. In countries with limited fiscal space, like most in Africa, making considerable gains in leadership – through the right choice of leaders or building adaptive leadership capacity – is easier than achieving comparable increases in fund allocation. Indeed, investing in excellent leadership can unlock additional resources from diverse internal and external sources. We can, therefore, correctly argue that leadership, specifically adaptive leadership, is the most important input for health systems in low-resource contexts.
HS 2.0 practitioners advocate for and provide technical assistance to political leaders, including presidents, prime ministers, and kings, to inform the reasonable allocation of funds to health within a country’s or administrative unit’s fiscal capacity. Equally crucial is encouraging political leaders to appoint individuals capable of, or willing to learn, adaptive leadership to key positions such as Minister for Health, Principal Secretary, and Director-General of Health. These top leaders, in turn, need to support training and/or mentorship for heads of directorates, divisions and sub-national health managers on the practice of adaptive leadership.
Practice #3 – Invest in Eight Interdependent Processes Through a People-Centered Lens
Premised on Systems Theory [2, 3, 4, 5], an effective health system that can deliver population health outcomes requires investing in eight interdependent processes that encapsulate the six building blocks of the 2007 WHO health systems framework [6], situated within the context of systems thinking and human-centered design. These processes are: finance management, human resources, medicines and commodities, medical equipment, community engagement (including young people and those with lived experience), multi-sectoral collaboration, digitization and digitalization, and integrated health services through models of delivery that are convenient for communities. When a health system effectively deploys these eight processes, it can achieve key functional attributes, namely access, equity, safety, quality, efficiency and responsiveness, leading to better coverage, financial protection and equitable gains in population health.
While Systems Theory has its successes, it is not a cure-all. The sub-systems are like a chain, vulnerable at the weakest link. Overlooking their interconnectedness leads to an inefficient equilibrium, which usually arises because efforts to improve one or more processes are neutralized by the weakest process in the system. For example, how often do we advocate for more resources for the health sector in the severely constrained fiscal spaces of African countries without an equivalent or stronger push for greater investment in preventive health interventions, which are highly cost-effective in the medium and long term and are possibly the most sensible way to invest most of the additional financial resources? Another example is how often we discuss data analysis without realizing that the power of data lies not in the analysis but in the curated causal insights on coverage and population health being publicly visible to communities and their leaders, who hold political power and influence to allocate resources and make other decisions, such as key staff appointments? A third example, as elaborated elsewhere in this paper, is that increasing skilled attendance at deliveries without commensurate gains in health worker skills and behavior or availability of life-saving medical supplies and equipment, often fails to lead to the expected reduction in the maternal mortality.
Integrating systems thinking (to connect the multiple cogs in a health system) with adaptive leadership (to catalyze system efficiency and offer leadership for change when inefficient equilibrium sets in – see Practice #6) and human-centered design (to prioritize people’s needs across the eight processes) can enable us to build efficient systems optimized to deliver population health outcomes.
Human-centered design, also known as people-centered design, focuses on tailoring solutions to meet the specific needs and contexts of communities rather than the preferences of the designer [7, 8]. It involves empathizing with communities to understand their needs, defining problems clearly, ideating and prototyping solutions, testing with communities, and iterating based on feedback. This approach ensures that health solutions are customized to meet real community needs in terms of access, equity, quality, affordabilit and responsiveness. Examples of human-centered design within health systems include the Better Immunization Data initiative in Tanzania and Zambia [9], the Aravind Eye Care System in India [10, 11], the Kimormor One-Stop-Shop outreach model in Kenya integrating animal health and human health [12, 13], low-cost solar-enabled movable clinics [14] delivering COVID-19 vaccines and other essential services to remote or hard-to-reach areas of Kenya, and the surgical training program for clinical officers in Malawi [15].
Practice #4 – Strengthen Health Governance as a Foundation for System Control
Health Systems 2.0 practitioners put significant effort into strengthening health governance, including laws, policies, regulations, strategies and coordination mechanisms that create an inclusive, enabling environment for health systems to protect and advance population health accountably and sustainably. As mentioned under Practice #1, HS 2.0 practitioners often find that their opportunity to strengthen governance lies in supporting electioneering political parties to define fit-for-purpose governance priorities in their manifestos and helping governments implement and improve performance based on measurable results and citizen feedback. Additionally, they coach managers to incorporate ‘controls’ to ensure the health system, in day-to-day operations, remains consistent with established governance frameworks. Such controls include costed work plans or roadmaps; monitoring frameworks that include measures of efficiency, equity, access and quality of care, as well as proxy indicators for population health; financial checks and balances; regular service audits that generate causal insights; tracking of performance metrics through dashboards or visualizations for leaders and communities to engage with; quality controls, including certification and accreditation standards for various cadres of health workers; and risk management measures, especially with reference to factors and trends in the health system’s operating environment, as described in Practice #7. Notably, HS 2.0 practitioners emphasize social accountability, whereby communities, including young people and those with lived experiences, track and hold duty bearers accountable for implementing governance and control mechanisms such as laws and policies.
HS 2.0 practitioners are adept at circumventing common traps, such as the false yet intellectually appealing dichotomy between a “systems approach” and a “vertical or disease program” approach. When funding exists for a vertical or disease program, HS 2.0 practitioners do their part to inspire and coach teams to use vertical program resources to strengthen the eight system processes for desired program results. For instance, a PEPFAR-funded HIV care and treatment program can transition peer educators to join the government-funded community health workforce, providing a broader scope of primary health care services that include health education and screening in addition to HIV-specific services. Similarly, development agencies can include systems strengthening objectives in the design stage of new programs, just as The Global Fund to Fight AIDS, TB and Malaria incorporates health system resilience-building in its country-led programs. This approach allows one to see the path that the dollar takes from the time it is released to strengthen the system, all the way to the desired population or patient-level outcomes.
HS 2.0 practitioners also coach teams and development partners who finance systems-strengthening programs to define some of the results in terms of population health. For example, an initiative addressing one or more of the eight processes, or two core inputs, or governance, or even informational feedback loops, can design a theory of change that describes population health as the ultimate goal, with intermediate results focusing on coverage, financial protection, the availability of financing for PHC services and the quality of health services provided.
Practice #5: Deploy Precision Population Health to Prevent ‘Inefficient Equilibrium’
To build insightful feedback loops, HS 2.0 practitioners inspire and guide teams to undertake thoughtful interpretation of reports or additional analysis of data from national surveys, existing health information systems and surveillance data. These informational feedback loops, if articulated as publicly visible and actionable insights or foresight, ought to guide adjustments in governance and control actions, resource allocation, leadership approaches as well as the eight processes. Notably, HS 2.0 practitioners help governments avoid ‘inefficient equilibrium’ by using real-time proxy indicators of population health to inspire stakeholders to take spot-on action. They coach teams to practice precision population health by identifying proxy or actual measures of population health and prioritizing daily work based on insights or foresight from such data.
For instance, in Kenya, skilled birth attendance more than doubled from 42% in 1998 to 89% in 2022, approaching universal coverage. Maternal deaths declined from 590 to 355 per 100,000 live births, a decrease of 40% during the same period. This improvement in maternal health falls short of expectations, given that 9 out of 10 mothers now trust health facilities for delivery. However, the health facilities have not been able to meet the expected quality of care. Health Systems 2.0 practitioners can address such gaps by supporting or coaching teams at sub-national levels to include proximate population health insights as part of real-time or monthly feedback, alongside quality-of-care insights. By coupling real-time proxy data on maternal health, such as facility maternal deaths, with quality-of-care data and correlating these measures at the client level through well-facilitated maternal death reviews, practitioners can continually uncover cost-effective system improvement opportunities. If addressed at the facility level through daily and weekly adjustments of patient care practices, as well as at sub-national and national levels by creating supportive environments, such opportunities are likely to lead to positive changes in maternal health. The application of precision population health could help initiatives like the Ending Preventable Maternal Mortality action plan achieve meaningful results.
Such a move would protect the health system from falling into an inefficient equilibrium caused by a failure to appreciate the system’s complexity. One remedy for inefficient equilibrium is the application of precision population health, where practitioners discover and deploy minimalist system improvement pathways that are efficient and informed by data to address prioritized health needs. This minimalist approach (or precision population health) can help nations and sub-national administrative units avoid the trap of attempting to transform every aspect of the health system with limited resources, such as Africa’s $54 total per capita expenditure on health, with government health expenditure averaging US$14.8 per capita. The minimalist technique shifts teams from ‘problem paralysis’ – where the problem seems so big and resources so limited that all one can do is advocate for more, often non-existent, resources – to a thoughtful focus on contextual solutions. While some may argue that population health is a lagging indicator that cannot be measured regularly and thus is not a good measure to inform weekly and monthly facility or community-level improvement actions, HS 2.0 practitioners need to offer leadership to iterate this view. They need to coach teams to learn to estimate population health changes through proxy real-time or monthly data. Promoting the use of proximate population health data offers nations with significantly constrained fiscal spaces a fair chance to deploy precision population health in both disease and vertical programs for better population health.
To illustrate why we need to keep innovating for real-time proxy measures of population health, consider this: Imagine running your company without knowing its profitability (a lag measure) for five years, the usual duration between population-based health surveys. Imagine that you only track sales or other lead measures during that time. This would be catastrophic for everyone working in the company, as well as the shareholders, as the company sinks, just like the Titanic, due to a lack of timely data on its financial health. In company settings, we avoid this deadly trap by using monthly or quarterly profit-and-loss statements (or income statements). These statements serve as a reliable proximate guide to determine if we are heading in the right direction. They inform our daily decisions and enable company executives to provide dependable quarterly updates to boards on how well the company is progressing toward long-term goals, such as increasing shareholder wealth. We need to apply similar thinking and action in the health sector to advance population health. If each nation does this, we will gradually steer the national health ships – with billions of people on board – out of harm’s way.
Practice #6 – Practice Adaptive Leadership Irrespective of Your Title or Position
A key skill and practice for HS 2.0 practitioners is adaptive leadership – leadership being a practice that anyone can learn, not a title or position. By practicing adaptive leadership, HS 2.0 practitioners can inspire the adoption of new practices, such as the eight described in this paper, by stakeholders in the broad health ecosystem. Considering the magnitude of such an ecosystem-wide scope, HS 2.0 practitioners can only be catalysts for change.
In a nutshell, HS 2.0 practitioners can practice adaptive leadership by distinguishing between adaptive challenges, which require leadership, and technical problems, which do not [16]. Confusing the two is a common cause of leadership failure. Technical problems, like a tumor requiring a surgeon to perform a surgical operation, can be resolved with existing knowledge. Conversely, adaptive challenges, like a persistently high maternal mortality ratio, teenage pregnancy rate or low coverage with financial protection, exist within a complex socio-political ecosystem of organizations and individuals with varying interests, values, motivations and knowledge. The persistence – without significant gains – or worsening of a health challenge at the population level despite multi-year remedial actions is possibly the most accessible proxy marker of adaptive challenges (as opposed to technical challenges) in the health sector.
Adaptive leadership practitioners address adaptive challenges by empathetically helping people learn and adjust to change that challenges their familiar reality and takes them outside their comfort zone. This includes coaching people to manage the loss that often comes with change, fostering a culture of observation, experimentation, and learning, creating the right amount of discomfort to stimulate learning while maintaining a supportive holding environment, and aiding the development of adaptive solutions by engaging and coaching a diverse set of stakeholders to participate in a contextual diagnostic process that unravels the problem’s ecosystem and bases desired change on what currently works. The contextual diagnosis entails a process to understand the problem’s ecosystem by identifying stakeholders, appreciating their perspectives, clarifying their desired outcomes, and noticing instances of positive deviance, where parts of the system work, and coaching stakeholders to enhance their adaptive leadership capacity to drive change while preserving what works as a firm foundation. The practice of adaptive leadership demands self-awareness, presence, deep listening, genuine engagement with others and self-care to avert exhaustion and burnout because it can be difficult and hard work.
To learn more about adaptive leadership, you can buy and read the book by Professor Ronald Heifetz et al., titled The Practice of Adaptive Leadership, which is a hands-on, practical guide (buy it on Amazon here – https://a.co/d/aQX6RRz).
Practice #7 – Embrace Factors or Trends in the Operating Environment
Health Systems 2.0 practitioners play a pivotal role in guiding ecosystem players to discern eight critical environmental factors and trends that necessitate adaptability in health systems strengthening work. These factors include climate change, the risk of pandemics and large-scale outbreaks, advancements in digitalization such as artificial intelligence, constrained financial resources exacerbated by the external debt situation, demographic dynamics like the youth bulge, epidemiological shifts such as the surge in cardiometabolic disorders across Africa, domestic and international conflicts, and the impact of migration and trade on health systems. Failure to acknowledge or recognize these environmental factors or trends within the operational landscape often leads managers to underestimate system complexity in their quest for simplification, impeding effective control and leading to the failure of health systems to deliver population health outcomes.
While one way to view the eight factors is through a risk management approach, considering that these factors often pose significant risks to the success of health systems, panother equally meaningful lens is that of opportunity. For example, even as we address the risks of climate change on health, such as through improved pandemic preparedness, we can also leverage climate funds to accelerate gains in high-impact climate/health adaptation measures, such as progressing toward the elimination of malaria, a climate-sensitive disease, as a public health threat. Similarly, imagine the gains we can achieve if we optimize the application of digitalization, such as Artificial Intelligence and Machine Learning, to discern insights from big data in national health information systems or to build forecasting models that enable us to manage uncertain and complex issues, such as determining investment choices for climate/health or programming for cardiometabolic diseases.
The eight environmental factors or trends are like waves in the ocean. HS 2.0 practitioners, who are the captains of the health systems boat, can benefit from a wave in the ocean by surfing or riding the wave. However, if a wave is moving against the boat’s direction, it can slow the boat down and make navigation quite difficult, and sometimes lead to catastrophic consequences. In the same way that sailors and captains often use their knowledge of waves to optimize their routes, HS 2.0 practitioners are encouraged to notice the eight types of waves, study them, and offer leadership to help steer health systems in ways that stand a good chance of delivering desired population health results. Sometimes, if the sea is too rough, like in the case of tsunamis that destroy everything in their path, HS 2.0 practitioners need to help stakeholders learn when to abandon the boat and adopt different transportation options, such as flying.
A good example of shifting gears from sailing to flying in the health system includes the potential for large-scale adoption of preventive interventions ‘to manufacture health at home at scale,’ powered by community health workers. Such a shift could enable low- and lower middle-income nations to weather the constrained fiscal space dilemma, often complicated by the threats of the external debt situation, the cardiometabolic disease epidemiologic trajectory, the effects of climate on health, and the emergence of pandemics and large-scale outbreaks. What other examples of shifting from sailing to flying can you think of?
Practice #8 – Embrace a Reformist Mindset
Health Systems 2.0 practitioners routinely advocate for, push, and negotiate health system reforms at all levels, promoting progressive practices to improve health outcomes. They champion reform initiatives at sub-national, national, regional and global levels, embracing leadership without requiring official titles. They refuse to confine themselves to the limits of frameworks or practices that have not delivered the desired results because they know that doing so is a form of white-collar insanity. Instead, they drive meaningful health system reforms from any position, taking individual and team action to drive change and leveraging available financial and network resources wherever they are. Additionally, they recognize that the cumulative impact of our collective small efforts, such as incorporating novel ideas like the HS2.0 philosophy into our current roles, has the potential to lead to the change we aspire to see. They are, therefore, not afraid of making small steps toward the change they envision, building on their current project’s or organization’s sphere of influence in the health ecosystem. Often, the initial small step is taking an interest in learning and understanding the health ecosystem or developing their skills in adaptive leadership.
HSm2.0 practitioners embrace the reformist mindset wherever they work. If they work with the WHO, they can facilitate, mediate, broker, and provide technically sound guidance for countries to customize their health systems to contemporary contexts, acknowledging that what we did to get to the stagnated UHC index will not get us out of the rut. They are not afraid to ask themselves what a new health systems framework would look like. Deep in their minds, they know that the WHO should consider convening a high-level dialogue on health systems to take stock of progress since 2007, when the current health systems framework was born, and lead the way in charting a path to the next fit-for-purpose version, aligned with the philosophy of PHC as the programmatic engine of UHC.
HS 2.0 practitioners who work with the government at managerial level know that they are well-placed to embrace adaptive leadership and allocate reasonable amounts of funds as core inputs for robust health systems, central to the Health Systems 2.0 philosophy. If they work with bilateral or multilateral development organizations, global health partnerships or philanthropic foundations, HS 2.0 practitioners are often keen to invest in meaningful impact pathways by applying their technical assistance and financial aid to grow the practice of adaptive leadership and data-driven performance improvement in health systems. Regarding performance measurement and improvement, they are able to simultaneously focus on short-term results, such as service quality and coverage and financial protection, and medium to long-term population health measures, such as disease incidence, prevalence, and mortality, correlating the two sets of measures on an ongoing basis to spur precision population health action.
Health Systems 2.0 practitioners who work in civil society need to always remember that they represent community interests and should, therefore, work collaboratively with other organizations and governments to follow three meaningful pathways, ensuring that the voices of communities are at the core of conversations and action about health system reform. First, they need to drive meaningful innovation capable of bending upward the currently plateaued UHC index trajectory. Second, they can advocate for the early implementation of evidence-based and effective health system models, including the at-scale adoption of forward-looking practices, some of which are described in this paper. Third, they can facilitate strategic discussions on health system reform with government ministers, WHO, academia and philanthropic foundations, as well as bilateral and multilateral agencies during key global health events such as the Africa Health Agenda International Conference, the World Health Assembly, and the United Nations General Assembly.
Health Systems 2.0 practitioners in academia can contribute to health systems reform by finding and presenting evidence on the efficacy of the current health systems framework and potential health systems reforms, particularly in lower-income countries. At this time, universities that teach public health and primary health care need to do more on implementation science to generate evidence on contextually relevant and scalable models of PHC to reorient health systems and upwardly bend the plateaued UHC trajectory. Additionally, such institutions need to train and mentor their students to practice adaptive leadership within the contexts in which they hope to work. In other words, these institutions need to nurture and mentor courageous health system reformists.
Health workers who embrace HS 2.0 practices need to deliver excellence in implementation at the frontline, employing adaptive leadership and human-centered design to address persistent health challenges across the eight sub-systems or processes at the local level, collaborating with local stakeholders.
Concluding Reflections
In our efforts to reorient health systems using the PHC approach, we have an opportunity to re-envision them as Health Systems 2.0 by applying Systems Theory, human-centered design and adaptive leadership to strengthen resilience and improve population health outcomes. Embracing Health Systems 2.0 offers hope that by thinking and acting differently based on UHC data trends, we can expedite progress toward SDG 3. This will bring more meaning to our work and resonate with communities, who can see and feel the results in better coverage and health outcomes.
A health development practitioner with experience in Africa’s maternal and newborn health recently said, “We have a short window of trust to show women that when they seek care at public health facilities, they will come out alive with a healthy baby.” What action, big or small, will you take on Monday to reform the health system at the level where you are working? Your action means everything to a mother, a newborn, a family, a community. Remember the eight HS 2.0 practices, eight interdependent processes, and eight critical factors in the operating environment. It’s like a game ofTriple Eight.
References
- Tracking Universal Health Coverage: 2023 Global monitoring report. Geneva: World Health Organization and International Bank for Reconstruction and Development / The World Bank; 2023. Licence: CC BY-NC-SA 3.0 IGO.
- Bertalanffy LV. General System Theory; Foundations, Development, Applications. New York: G. Braziller; 1969.
- Paina L, Peters DH. Understanding Pathways For Scaling up Health Services Through the Lens of Complex Adaptive Systems. Health Policy Plan. 2012 Aug 1;27(5):365–73.
- Braithwaite J, Churruca K, Long JC, Ellis LA, Herkes J. When complexity science meets implementation science: A theoretical and empirical analysis of systems change. BMC Med. 2018 Dec;16(1):63.
- Straub R. Why Managers Haven’t Embraced Complexity. Harvard Business Review. 2013. https://hbr.org/2013/05/why-managers-havent-embraced-c. Accessed 15/3/2024
- Everybody’s Business: Strengthening Health Systems to Improve Health Outcomes – WHO’s Framework for Action; World Health Organization, 2007.
- IDEO.org. The Field Guide to Human-Centered Design. 2015. Canada. IDEO.
- Huffman K. The key to better primary health care? Human-centered design. 2019. https://www.path.org/our-impact/articles/key-better-primary-health-care-human-centered-design/. Accessed 12/03/2024.
- Mvundura M, Di Giorgio L, Vodicka E, Kindoli R, Zulu C. Assessing the incremental costs and savings of introducing electronic immunization registries and stock management systems: Evidence from the better immunization data initiative in Tanzania and Zambia. Pan Afr Med J. 2020 Feb 12;35(Suppl 1):11. doi: 10.11604 pamj.supp.2020.35.1.17804. PMID: 32373262; PMCID: PMC7195915.
- Lewallen S, Thulasiraj RD. Eliminating cataract blindness – how do we apply lessons from Asia to sub-Saharan Africa? Glob Public Health. 2010 Nov;5 (6):639–48.
- Saqib, N. & Mathu, A. A. (2024). Frugal Business Model Innovation in an Indian Emerging Market: A Case Study of Aravind Eye Care System. In V. Gupta (Ed.), Fostering Global Entrepreneurship Through Business Model Innovation (pp. 184-205). IGI Global. https://doi.org/10.4018/978-1-6684-6975-0.ch007
- Amref. Where families and their animals are treated in one clinic (Reported by Angela Oketch, Nation Media Group). 2021. https://newsroom.amref.org/news/2021/01/where-families-and-their-animals-are-treated-in-one-clinic/. Accessed 12/03/2024
- Amref. One Health Approach Strengthens Human and Animal Health in Turkana, Kenya (Reported by Kevin Majoni, Communications Lead, USAID Imarisha Jamii). 2024. https://newsroom.amref.org/blog/2024/03/one-health-approach-strengthens-human-and-animal-health-in-turkana-kenya/. Accessed 17/08/2024
- Amref. Ministry of Health, Kenya in Partnership with Amref Health Africa and AstraZeneca Rolls out Mobile Clinics to Boost Covid Vaccines Uptake. 2022. https://newsroom.amref.org/news/2022/07/moh-rolls-out-mobile-clinics-to-boost-covid-vaccines-uptake/. Accessed 12/03/2024
- Gajewski J, Borgstein E, Bijlmakers L, Mwapasa G, Aljohani Z, Pittalis C, et al. Evaluation of a surgical training programme for clinical officers in Malawi. Br J Surg. 2019 Jan 8;106(2):e156–65.
- The Practice of Adaptive Leadership: Tools and Tactics for Changing Your Organization and the World by Ronald Heifetz, Alexander Grashow, and Marty Linsky. Pers Psychol. 2010 Mar;63(1):255–8.
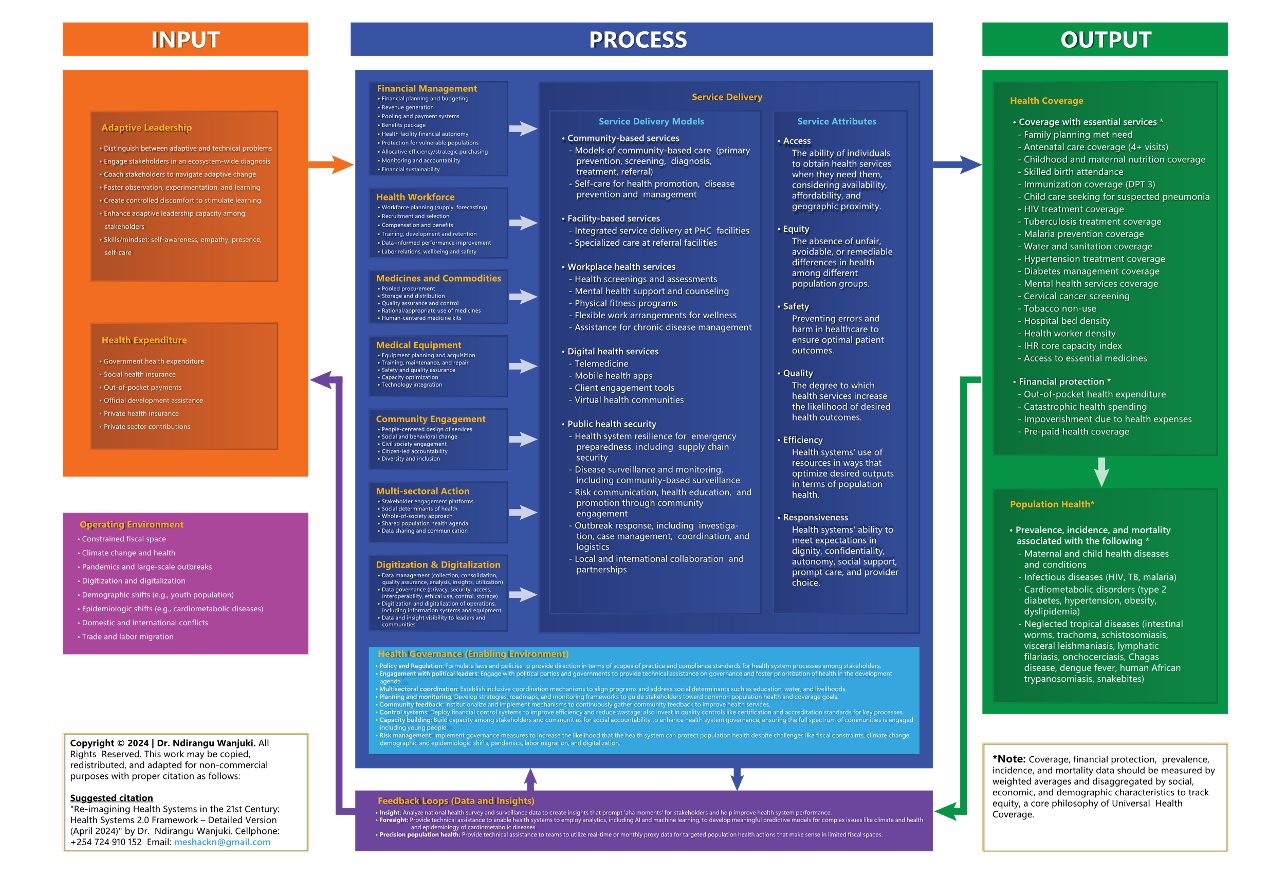
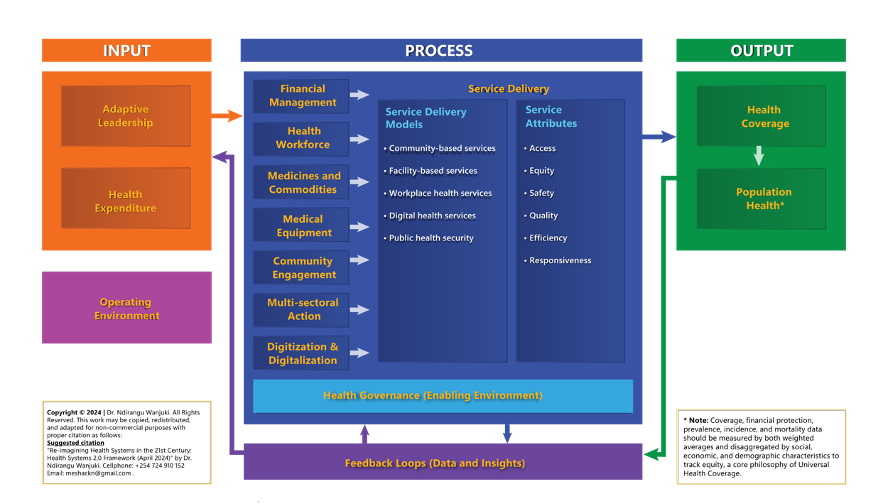
Annex 1: Health Systems 2.0 Framework Founded on System Design, Human-Centered Design and Adaptive Leadership (Simplified Version)
Annex 1: Health Systems 2.0 Framework Founded on System Design, Human-Centered Design and Adaptive Leadership (Detailed Version)